.jpg)
Case of the week 17 (
December 2011
)
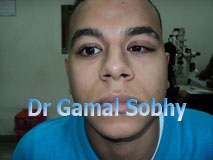
Huge Consecutive Exotropia
|

This 21 years old young man has a history of what
appears to be congenital esotropia. I assume it was
a large angle congenital esotropia since he had a bimedial
rectus recession and Lt lateral rectus resection
when he was 6 years old ( Ugly conjunctival scars could be
seen medially and Lt laterally by the naked eye )
. Although 3 muscle surgery had been done , a small
residual esotropia appeared soon after the operation
, he was advised to wear glasses in order to correct
the residual angle , this was incorrect as shown in
the old pictures of the patient .
This year ( 2011 ) the patient ended his university study
, now he is a biochemistriest ,
he wants to attach the Egyptian Military Forces , he
was informed that the residual esotropia should be
corrected first .
He underwent Right lateral rectus resection 2 months
ago. This surgery resulted in a large angle left consecutive exotropia
, the patient is referred to me , he is very
tempered and very angry about the huge exotropia
after this surgery
VA
is 6/6 OD 6/6 OS aided
with +0.75 sph both eyes
|
|
11 years old |
13 years old |
18 years old |
.jpg) |
.jpg) |
.jpg) |
Many years of working on such complicated cases
where prior surgeries were done , the surgeons
are not known , the operative details are exactly
unknown and the results are not good
taught me it is best to deal with the patient more
of less as a "new" patient.
Based on the above, this young man has a huge Lt.
XT, slight limitation of adduction OS and what looks
like a scarred conjunctiva , the 2 MR are possibly
recessed and the 2 LR are possibly resected.
These cases require decisions be made in the
operating room depending on what is found and on the
operative scinario.
I did a large recession for the
previously resected left LR putting the muscle at or
very near the equator with upshift to correct the V
pattern. I found the lateral conjunctiva is
tight , so I slightly recessed it. Then I advanced
and resected the previously recessed Lt MR left
medial as much as I can without pulling forward
tissues of the medial orbit , the MR is sutured
nearly at its original insertion ( 5.5 mm of the limbus )
with downshift to correct the V pattern
In cases like this, the big challenge of the surgeon
is the fibrosis of the periorbital tissue, I always be sure to do forced ductions before and after detaching the
muscles to asses this fibrosis . Fibrosis of the
periorbital tissue is the main cause of limited
ductions following previous orbital surgeries, it is
also the main cause of disappointing undercorrection
of these patients . So, forced ductions will
be a clue as to what you can expect from this part
of the operation. Also, be sure to avoid inclusion of the inferior oblique
in the left lateral rectus.
Finally , I've found the medial conjunctiva is tightly
scarred , I've recessed it .
|
|
|
Post operative
the day after
|
|
 |
 |
 |
 |
 |
 |
 |
 |
 |
|
|








