.jpg)
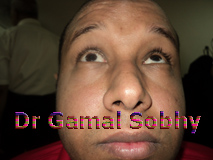
Case of the week 135 ( September 2013 )
Partial
third nerve palsy
|
 |
35 years old patient complains of sudden
onset of diplopia 2 months ago. No history of
trauma, no history of fever or any general
illness. MRI brain and orbit was done, no
abnormalities could be detected. |
|
See video of this patient |
| |
Partial
third nerve palsy
Due to the separation of
the third nerve fascicles as they leave their
nuclear complex, pass through the red nucleus,
substantia nigra, and the pyramidal tracts to
exit the brainstem into the interpeduncular
fossa, damage in this region often results in
incomplete paralysis. The pupil may be spared,
or an isolated paralysis of elevation may be
found. Even patterns of isolated superior or
inferior divisional palsies of the third nerve
can arise from disease located within the
midbrain. Associated deficits of additional
midbrain structures are likely to be found,
including vertical gaze pareses (damage to the
rostral interstitial nucleus of the medial
longitudinal fasciculus), bilateral ptosis
(typically present with lesions of the third
nerve nucleus), paralysis of convergence and/or
accommodation, and loss of all contralateral
somatic sensation . Most fascicular pareses are
ischemic in origin, and are only occasionally
the result of infiltrating of inflammatory
processes. Microvascular ischemia of the
oculomotor nerve arises from small-vessel
disease of the vasa vasorum supplying the third
nerve. It is the most common cause of oculomotor
paresis in most ophthalmic practices. Though not
specific, the presentation is characteristic,
including acute onset of diplopia, complete or
partial palsies of the muscles supplied by the
third nerve, sparing of the pupillary sphincter,
and ipsilateral retrobulbar and/or temporal
pain. The pain is thought to stem from the acute
inflammatory response to the infarcted nerve
within the subarachnoid space, i.e., a locus of
sterile meningitis. The pupillary sparing
reflects the surface location of the autonomic
fibers, providing some oxygen supply via the
cerebral spinal fluid. The fibers are also small
and have lower metabolic requirements than the
larger, more quickly conducting oculomotor
fibers. It also explains their greater
susceptibility to compressive lesions
Simultaneous damage to the sympathetic fibers in
the cavernous sinus can also conceal damage done
to the pupillomotor fibers by minimizing the
resultant mydriasis. Vasculopathic oculomotor
cranial nerve palsies are most common in
middle-aged and elderly patients. The paresis is
monocular, and typically, other cranial nerves
are not affected. A spontaneous recovery is the
rule, taking 4 to 6 months for completion. The
diagnosis can initially be difficult. During the
first 10 days, there may be a staircase
progression of additional motor loss, which
happens in more than half of all cases. Risk
factors for this type of small-vessel disease
include age, diabetes mellitus, hypertension,
and generalized arteriosclerosis. Relapses in
the same or other ocular motor nerves are not
uncommon. More than one nerve can be involved at
the same time and problems can appear
bilaterally, but these are uncommon events. The
diagnosis is difficult to confirm initially, but
it is ultimately proven by the subsequent
recovery.
|
|
|
|