.jpg)
Case of the week 162 ( February 2014 )
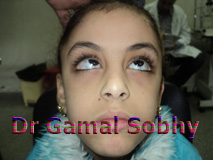
V pattern esotropia
|
 |
7 years old girl was noticed by her parents
to have inward eye deviation since early
childhood, the girl herself complains of sever
asthenopia following reading and any near work.
vision is 6/6 OD 6/6 OS
Cyclorefraction : -0.25 cyl 90 OD
-0.25 cyl 90 OS |
V pattern esotropia
One of the most valuable contributions in the
second part of the twentieth century to the field of
strabismus was the emphasis on what has come to be known
as the A and V
patterns of
strabismus.
How the
existence of A or
V
patterns could have escaped the
attention
of ophthalmologists until so recently.
This
girl has a ‘V’ pattern congenital esotropia.
Asthenopia is a common complaint
in patients with
V
pattern ET, since fusion may have
to be maintained for a long time in certain positions of
gaze. The increase in a deviation in downward gaze in
V
esotropia
may cause visual discomfort during reading or other
types of near work.
Also note the antimongoloid fissure which could be associated with pulley
heterotopy. In this case the medial pulleys would be
displaced upward and the lateral pulleys displaced
downward. According to the pulley theory, the ‘V’
pattern is caused by the vertical displacement of the
horizontal rectus muscle action. Of Course pulley
displacement must be confirmed by coronal imaging of the
mid-orbit, but this is not readily available because of
cost . The traditional treatment for a case like this is
bimedial rectus recession with bilateral inferior
oblique weakening. However, some cases treated this way
have persistent overaction of the inferior obliques.
This could result from unrecognized, or untreated,
pulley displacement contributing to the vertical
incomitance. Combined inferior oblique weakening and
down shift of the recessed medial recti could also be
done. As an extreme, weakening of the inferior obliques
and tuck of the superior oblique, if they are loose,
could be done along with bimedial rectus recession, but
I think that is too much surgery for this girl.
My decision here is to do BMR rec with downshift +
Bilateral IO myotomy ,
See the patient
24 h Post operative
|
|
|
|