|

Strabismus course : 17. Decision
making
In a case like this the
ophthalmologist should be aware of different causes of
limitation of depression of one eye (
The above slide contains these causes )
and should be able to differentiate
between restrictive causes from other causes .
Mechanical
causes that interfere with depression of the eye
must be excluded.
In spite of absence of history of previous orbital
surgery or orbital trauma in the accident which may
exclude restrictive causes , forced ductions must be
done to rule out this .
Double Depressor Palsy ( DDP )
This is one of the most rare
oculomotor disorders may be seen by the strabismologist
all over his life . This is my third
case of DDP within 30 years of ocular motility examination . My
first 2 cases were congenital , this case is acquired most
probably due to central lesion following the sever head
injury although MRI and CT brain could not localize the
underlying pathology. Paralysis
of both depressor muscles of one eye (inferior rectus
and superior oblique) always occurs with obscure
etiology because both depressor muscles are innervated
from different nuclei ( 3rd and 4th ).
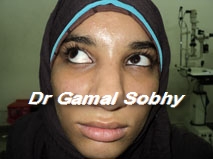
The characteristic ocular motility of DDP are : when the non-paretic eye is fixating, the paretic eye is hypertropic in primary position (Picture 5). . Ductions
are limited in the entire lower field of gaze and normal
in all other gaze positions.
Patients have double depressor
palsy are rarely found in the literatures , I have been
invited once to a session titled " a case of double
depressor palsy " . I put photos of my case in comparative with
the only case of DDP of the great text " Binocular vision and Ocular
motility " , I think they are the same with
different colors

Binocular vision and ocular
motility

Therapy
Knapp introduced vertical transposition of the
horizontal rectus muscles to the medial and lateral edge
of the superior rectus muscle insertion to treat
the double elevator palsy
(Knapp procedure) , an analogous approach is used
to treat a double depressor palsy : both horizontal
rectus muscles are transposed to the medial and lateral
edge of
the inferior rectus insertion ( inverse Knapp procedure
)
|
.jpg)