.jpg)
Case of the week 47 (
April 2012
)
Parasellar Meningioma
|

 |
 |
|
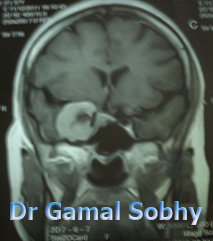
38 years old woman
complains of gradual diminution of vision Rt eye
since 3 months .
VA 6/24 OD , 6/6 OS
Fundus : hyperemic Rt optic disc
She was not aware of the obvious protrusion
of the right eye , MRI is asked and shows
this findings |
|
Parasellar tumors are
neoplasms that arising from the anatomical structures that
border the sella turcica. The sella with its
content, i.e. the pituitary gland, is imited
superiorly by the diaphragma sellae; laterally by
the dural wall of the cavernous sinus, a
multiloculated venous structure containing the
internal carotid artery, the cranial nerves III, IV,
VI, and the V1 and V2 branches of the trigeminal
nerve; inferiorly by the basisphenoid bone and
sphenoid sinus, posteriorly by the dorsum sellae.
The suprasellar subarachnoid space lies above the
diaphragma sellae, contains optic nerves and chiasm
and the infundibular stalk, and is defined
superiorly by the hypothalamus and anterior third
ventricle. The Gasserian ganglion region, although
it is not anatomically related to the sellar region,
can be considered a parasellar structure.
Pathology affecting the parasellar region can arise
from the pituitary gland, infundibular stalk,
hypothalamus, meninges, vessels, cranial nerves and
nasopharynx.
The
parasellar meningioma is located in the middle of
the base of the skull. The parasellar meningioma can
result in worsening vision. Surgical removal of
this meningioma is an option for relief of symptoms.
Radiosurgery is an important option for treatment of
the parasellar meningioma as well. Radiosurgery
should also be considered in an asymptomatic patient
if there is a likely probability of future visual
symptoms. When a large meningioma involves the optic
apparatus, internal carotid, or anterior cerebral
arteries with dense adherence surgery can have
higher risks.
The management of the parasellar meningioma
remains a challenge because of their poor surgical
accessibility and proximity to critical
neurovascular structures. Although advances in
cranial base surgical techniques have lowered
surgical mortality rates dramatically, postoperative
morbidity, especially in terms of new cranial
neuropathies, remains significant .
Stereotactic radiosurgery with the Gamma Knife is
a durable and minimally invasive option for the
treatment of parasellar meningiomas. It offers a
reasonable rate of tumor control and a low incidence
of new neurological complications. Smaller-volume
tumors appear to respond readily to radiosurgery.
Larger-volume tumors, however,
may
benefit from a cytoreductive resection prior to
radiosurgery.
Radiosurgery for the meningioma is recommended
when there has been a subtotal removal with an
inadequate decompression, or there is evidence of
recurrence on MRI after radical subtotal removal.
|
|
|